

Diabetes Before Insulin
When people learn that I eat a low carb, high fat diet and measure my ketones frequently, hoping that I have a measurable amount of ketones in my blood, they inevitably ask me, “Aren’t ketones dangerous to diabetics?” or “Can’t ketosis kill you?” It is a common misunderstanding where people confuse ketosis with Diabetic Ketoacidosis. This post is the first of three where I clarify the difference and dispel some myths.
If the last time you thought about peptic ulcers was prior to the 1980’s, your understanding of the disease is based on a consensus that it was a chronic, sometimes fatal disease caused by stress and the stomach overproducing acid, eating away its own lining. Then in 1983 a bacterial infection was definitively identified as the cause of peptic ulcers. From that point forward it physicians treated and cured it with a simple round of antibiotics. Yet to this day, people will caution you that too much stress can give you an ulcer. The next time you hear from someone that a ketogenic diet is dangerous, and could kill you, or that high fat diets will give you heart disease, I want you to bear this perspective in mind.
In this first post, I’d like to ruminate for a moment on the history at the root of our outdated fear of ketones. While the greatest minds in the history of diabetic research and treatment deserve reverence and thanks for their dedication and insight, it is important to recognize that their insights came from eras where our ability to measure biological markers and our understanding of the etiology of diabetes were more limited. Some misunderstandings took root over time and are still a part of our collective “wisdom” today even though they are not supported by the current scientific consensus.
Type 1 and Type 2 Siphon Sweet
T1 and T2 Diabetes Mellitus are two entirely separate diseases that share the same base name. This is because from ancient times until the first third of the twentieth century, they were both considered the same disease, expressing itself in different levels of severity. It was all just the sickness that some people would get, which would cause sugar to begin spilling into their urine. The actual label of diabetes means siphon or the disease where one’s flesh siphons out through the urine. In the words of the Greek physician, Aretaeus:
“[A diabetic’s] fluids do not remain in the body, but use the body only as a channel through which they may flow out. Life lasts only for a time, but not very long. For they urinate with pain, and painful is the emaciation. For no essential part of the drink is absorbed by the body, while great masses of the flesh are liquefied into urine.”
The correlation between sweetness of the urine and illness was first recorded when doctors in India noticed that the area where those afflicted with the disease urinated would attract ants, which fed off of the sugar after the urine had dried.[1] It also is sometimes attributed to the sweet smell of acetone on the breath of someone who can no longer process sugar and whose metabolism switches to the body’s fat stores for energy. Hence, label for diabetes was further categorized as diabetes mellitus, or “Siphon Sweet.”
Of course not everyone with sweet urine became emaciated and died quick, horrible deaths. Some people started expressing sugar in their urine later in life, without the diminishing girth (indeed, quite the opposite) but with the accompanying coronary disease, blindness, neuropathy, infection and kidney failure that is the hallmark of poorly controlled diabetes in either population. This was less of a problem in ancient history because Type 2 diabetes is more a disease of civilization where lifestyle removed from hunter gatherer activities allows for less activity and more refined foods in the diet.
For much of the recorded history of the disease, the variety of diabetes that afflicted mostly children (subcategorized as juvenile onset diabetes mellitus) and variety that afflicted mostly adults (adult onset diabetes mellitus) were considered at their root the same disease, which expressed itself with different levels of severity in different populations and vaguely had something to do with the pancreas. This distinction regarding the pancreas comes from experimentation in the late 1800s when Drs. Mering and Minkowski removed the pancreas of various lab animals only to watch them start spilling sugar in thier urine, and wasting away until they died.
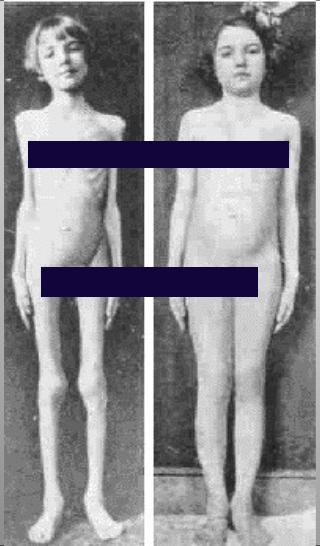
The reversal of emaciation of a T1 diabetic, before and after the discovery of insulin
Even when Dr. Frederick Banting and his research associate, James Best, isolated the “essence of pancreas” that lowered blood sugars in diabetics and named it insulin, no one had actually seen the insulin molecule or even understood the complicated role it played in one’s energy metabolism and homeostasis. It was simple enough that it lowered blood sugar to the point that it no longer spilled into the urine, reversed the physical wasting of those with the acute form of the disease, and seemed to improve the health outcomes of those with the less acute form.
The distinction that each form of diabetes were distinct and arose from different factors actually came from the work of Sir Harold Himsworth, MD, who developed the first glucose tolerance test. In 1936 he published the results of comparing glucose-tolerance scores of healthy people to those of both subcategories of diabetics. He determined that people had varying degrees of sensitivity to insulin. The so-called, Juvenile Onset Diabetics were just as sensitive as a normal, healthy person, while the Adult Onsets had insulin insensitivity. He further postulated that they were actually two entirely different diseases, one type where people lost their ability to produce insulin and a second type were people were insulin-resistant (a term which Dr. Himsworth himself coined). Then two decades later in 1959, Drs. Berson and Yalow devised a method to measure levels of insulin while still within a person’s body, leading to a confirmation of Dr. Himsworth’s hypothesis.
The actual labels “Type 1” and “Type 2” Diabetes Mellitus were first coined by John Lister, a physician in London in 1951, but did not gain favor until 1976 along with the terms Insulin Dependent and Non-Insulin Dependent Diabetes Mellitus (IDDM and NIDDM, respectively). Now the medical and research community use the terms Type 1 and Type 2 to refer to the two diseases exclusively.[2]
Ketone Danger is Greatly Overstated
Remember when I mentioned that the part of the moniker for our disease, mellitus, “…is sometimes attributed to the sweet smell of acetone on the breath of someone who can no longer process sugar and whose metabolism switches to the body’s fat stores for energy”? The acetone that causes that smell is one of three types of ketone bodies produced under those conditions.
Before the refinement and use of insulin in diabetic treatment in 1922, a juvenile diagnosis of diabetes was tantamount to a death sentence. A child who fell victim to the disease prior to the discovery of insulin would go through a brief honeymoon period as his or her insulin producing capability declined, where their body would eat itself and produce tremendous amounts of ketones to satisfy the child’s energy needs absent the ability to process glucose. This storm of ketones coupled with the high level of sugar hanging around in the blood stream would result in a condition known as Diabetic Ketoacidosis (DKA) and kill the child long before many of the other outcomes of poorly managed diabetes that we recognize today surfaced.
But the mere presence of ketones does not imply ketoacidosis anymore than a heavy fog implies a hurricane. The absence of enough insulin to control your blood sugars and to keep your fat cells from flooding your bloodstream with fatty acids is the difference that makes a difference.
I will go into detail about the progression of DKA in my next post. For the purposes of this installment, it is enough to understand that the presence of ketones in the blood, in the urine and on the breath of a diabetic was taken as a sign of impending doom and even after the discovery of insulin, a sign of poor control of the disease that would surely lead to a bad outcome. At a time when there was no differentiation between the two types of diabetes, the ketone became a boogeyman and never recovered, despite the years of further refined scientific distinctions to the contrary.
Part 2: Diabetic Ketoacidosis: A Study In Extremes
Part 3: Nutritional Ketosis: A Diabetic Ally In Disguise
[1] Depending on how much sugar you spill in your own urine, you may notice that your toilet bowl at home develops a black ring very easily at the water line. This is bacteria feeding on the rich sweetness that you’ve left behind.↩
[2] For an excellent summary and perspective on the differentiation between T1 and T2 Diabetes Mellitus, head on over to Diapedia. I found this resource while looking for John Lister’s original paper on glucose tolerance testing. Professor Edwin Gale goes into detail on how the name had its origins in the mid-twentieth century medical fascination with Somatotyping.↩